Bridging the Design-to-Manufacturing Gap in Medical Devices
TL;DR
- Design transfer should run throughout development, not just at the end.
- Early manufacturing involvement prevents redesigns and delays.
- “Fit-to-learn” builds are strategic only when temporary.
- Cross-functional collaboration drives scalability and quality.
- Continuous design transfer links innovation to market readiness.
Rethinking Design Transfer in Medical Device Development
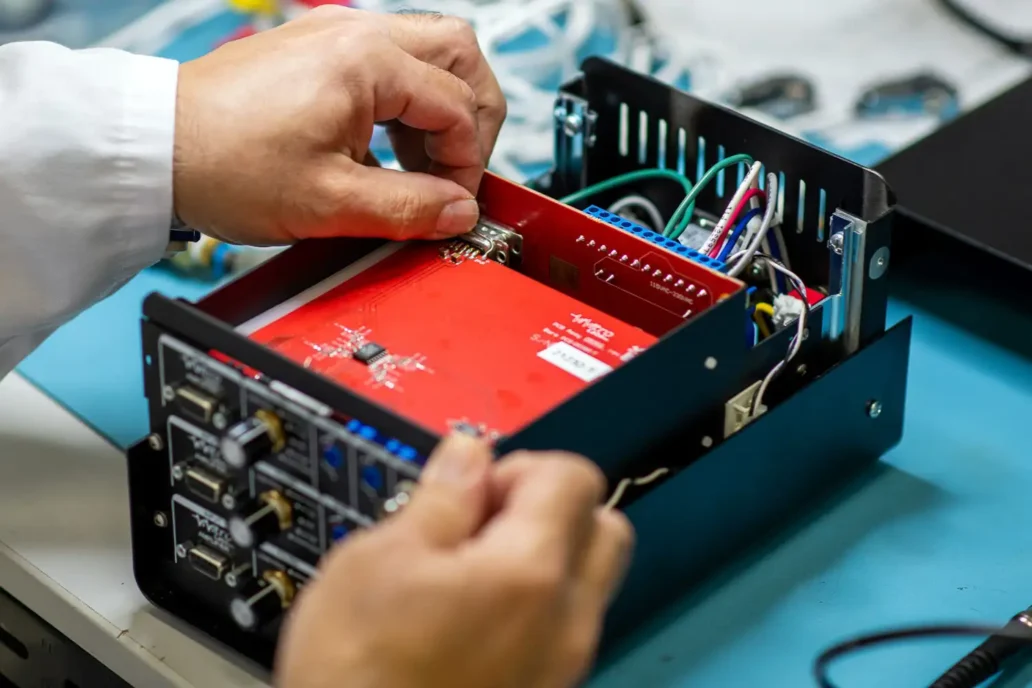
Your team is ready for design validation. The prototype performs well, test plans are in motion, and everything points to a smooth handoff to manufacturing. Then your partner calls with bad news: they can’t build the device as designed. Overnight, momentum shifts to damage control, bringing delays, redesigns, and rising costs. For many startups, setbacks like this push time-to-market beyond recovery, where technical progress stops translating into company value.
Many companies fall into this trap, treating design transfer as a final handoff before production instead of a bridge between development and manufacturing readiness. But here’s the catch: design validation units must be built in a production environment using real design outputs and quality controls. If manufacturability issues surface at this stage, it’s already too late.
When design transfer happens too late, teams face missed milestones, redesigns, and costly delays. Some organizations intentionally accept design compromises that raise costs or limit scalability. Early in a launch, that can be a strategic choice. These early “fit-to-learn” builds validate product-market fit and generate clinical or market feedback.
The key is to make those trade-offs consciously and temporarily, with a clear plan to refine the design once the value proposition and market alignment are validated. When compromises persist beyond early validation, they shift from strategic to constraining. even strong technologies stall when cost and scalability barriers limit market adoption.
Why Design Transfer Fails When Treated as a Handoff
Design transfer isn’t a single handoff at the end of development. It’s a continuous process that guides how a product moves from prototype to production. When teams wait too long to involve manufacturing, problems surface late, triggering redesigns and production delays. The result is a reactive scramble that erodes time, trust, and budget between development and manufacturing.
How to Integrate Manufacturing Early
Successful design transfer depends on who’s involved early. Design teams focus on ensuring outputs meet inputs (and rightly so), But they don’t always prioritize design for manufacturability. That’s where new product introduction (NPI) and manufacturing engineers add real value. Their perspective on how to build at scale, test on the line, and maintain devices ensures manufacturability is built in from the start.
Involving them early not only improves prototype design but also builds buy-in from the manufacturing team long before time pressure sets in. When development and production collaborate from the beginning, design transfer becomes a shared objective rather than a final hurdle.
Making Design Transfer a Continuous Process
Every decision made during development shapes how easily a product can be built, scaled, and supported. Integrating design transfer throughout these stages keeps teams aligned and prevents late-stage surprises that drain time and resources.
Treat design transfer as the thread that ties every stage of development together. When manufacturing insight shapes each iteration, teams move faster, avoid costly setbacks, and deliver products ready for real-world success.
Jasmine is an NPI Engineer with over 12 years of experience in medical device development. She specializes in late-stage design, turning early concepts into market-ready products.
Images: Adobe Stock
Related Resources

Nigel Syrotuck breaks down REACH SVHC compliance for teams working with material suppliers and compliance questionnaires.

We examine when computational modelling and simulation, or CM&S, genuinely supports medical device simulation strategy and when it becomes a costly detour.
Many teams still underuse CM&S, often bringing it late in device validation, when key decisions have already been made. That approach leaves much of the value of CM&S untapped.
This article traces the Pennes bioheat equation from its 1948 origins to modern multiscale approaches, explaining how engineers select the right level of modelling complexity across device categories.